Blank Texas Dwc069 PDF Template
Form Example
Texas Department of Insurance
Division of Workers’ Compensation
7551 Metro Center Drive, Suite 100
(800)
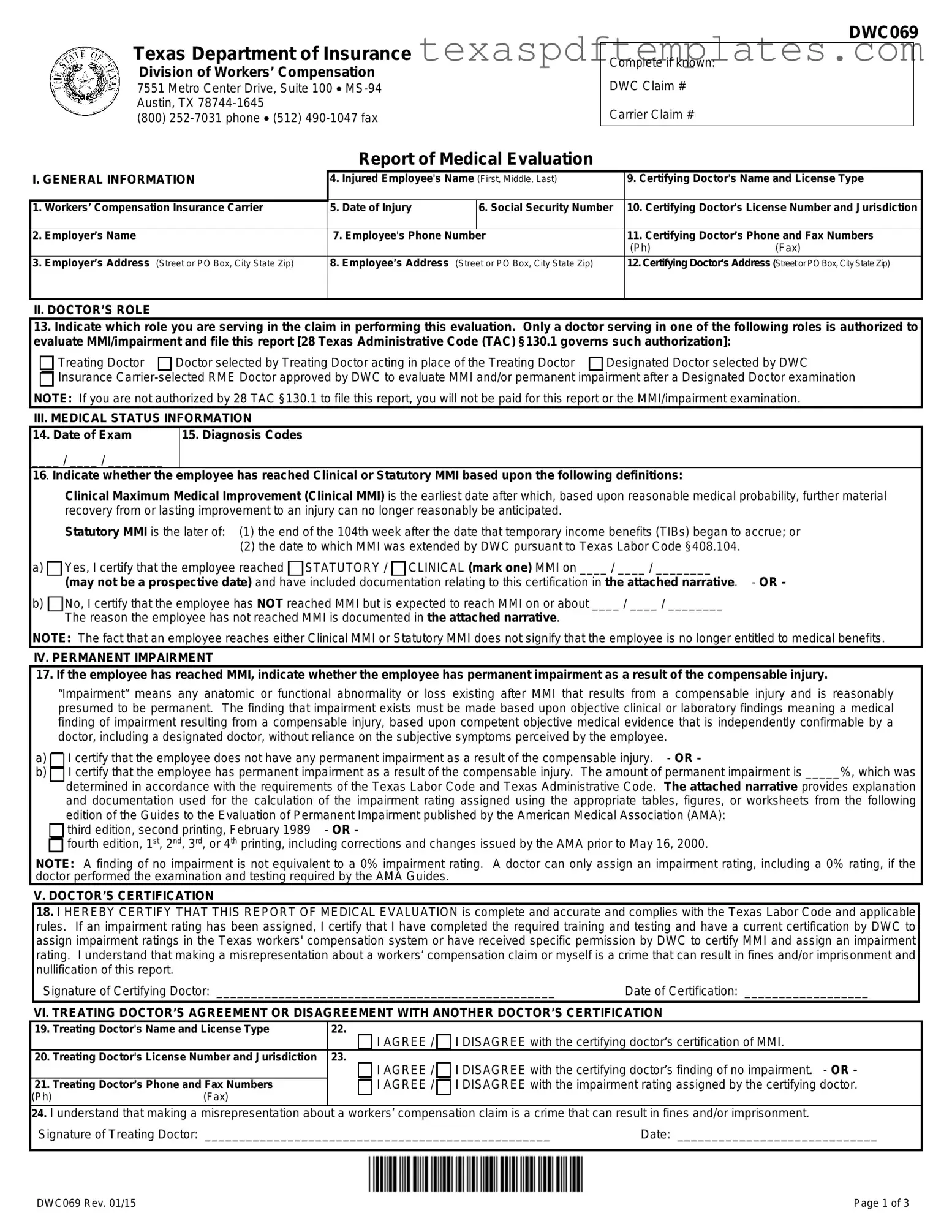
Report of Medical Evaluation
DWC069
Complete if known:
DWC Claim #
Carrier Claim #
I. GENERAL INFORMATION |
4. Injured Employee's Name (First, Middle, Last) |
|||
|
|
|
|
|
1. |
Workers’ Compensation Insurance Carrier |
5. |
Date of Injury |
6. Social Security Number |
|
|
|
|
|
2. |
Employer’s Name |
7. Employee's Phone Number |
|
|
|
|
|
|
|
3. |
Employer’s Address (Street or PO Box, City State Zip) |
8. |
Employee’s Address (Street or PO Box, City State Zip) |
|
|
|
|
|
|
9.Certifying Doctor's Name and License Type
10.Certifying Doctor's License Number and Jurisdiction
11.Certifying Doctor’s Phone and Fax Numbers
(Ph)(Fax)
12.Certifying Doctor’s Address (Street or PO Box, City State Zip)
II. DOCTOR’S ROLE
13.Indicate which role you are serving in the claim in performing this evaluation. Only a doctor serving in one of the following roles is authorized to evaluate MMI/impairment and file this report [28 Texas Administrative Code (TAC) §130.1 governs such authorization]:
Treating Doctor |
Doctor selected by Treating Doctor acting in place of the Treating Doctor |
Designated Doctor selected by DWC |

 Insurance
Insurance
III. MEDICAL STATUS INFORMATION
14. Date of Exam |
15. Diagnosis Codes |
____ / ____ / ________ |
|
16. Indicate whether the |
employee has reached Clinical or Statutory MMI based upon the following definitions: |
Clinical Maximum Medical Improvement (Clinical MMI) is the earliest date after which, based upon reasonable medical probability, further material recovery from or lasting improvement to an injury can no longer reasonably be anticipated.
Statutory MMI is the later of: (1) the end of the 104th week after the date that temporary income benefits (TIBs) began to accrue; or
(2)the date to which MMI was extended by DWC pursuant to Texas Labor Code §408.104.
a) Yes, I certify that the employee reached
Yes, I certify that the employee reached  STATUTORY /
STATUTORY /  CLINICAL (mark one) MMI on ____ / ____ / ________
CLINICAL (mark one) MMI on ____ / ____ / ________
(may not be a prospective date) and have included documentation relating to this certification in the attached narrative. - OR -
b) No, I certify that the employee has NOT reached MMI but is expected to reach MMI on or about ____ / ____ / ________
No, I certify that the employee has NOT reached MMI but is expected to reach MMI on or about ____ / ____ / ________
The reason the employee has not reached MMI is documented in the attached narrative.
NOTE: The fact that an employee reaches either Clinical MMI or Statutory MMI does not signify that the employee is no longer entitled to medical benefits.
IV. PERMANENT IMPAIRMENT
17. If the employee has reached MMI, indicate whether the employee has permanent impairment as a result of the compensable injury.
“Impairment” means any anatomic or functional abnormality or loss existing after MMI that results from a compensable injury and is reasonably presumed to be permanent. The finding that impairment exists must be made based upon objective clinical or laboratory findings meaning a medical finding of impairment resulting from a compensable injury, based upon competent objective medical evidence that is independently confirmable by a doctor, including a designated doctor, without reliance on the subjective symptoms perceived by the employee.
a) I certify that the employee does not have any permanent impairment as a result of the compensable injury. - OR -
I certify that the employee does not have any permanent impairment as a result of the compensable injury. - OR -
b) I certify that the employee has permanent impairment as a result of the compensable injury. The amount of permanent impairment is _____%, which was determined in accordance with the requirements of the Texas Labor Code and Texas Administrative Code. The attached narrative provides explanation and documentation used for the calculation of the impairment rating assigned using the appropriate tables, figures, or worksheets from the following
I certify that the employee has permanent impairment as a result of the compensable injury. The amount of permanent impairment is _____%, which was determined in accordance with the requirements of the Texas Labor Code and Texas Administrative Code. The attached narrative provides explanation and documentation used for the calculation of the impairment rating assigned using the appropriate tables, figures, or worksheets from the following
edition of the Guides to the Evaluation of Permanent Impairment published by the American Medical Association (AMA): 
 third edition, second printing, February 1989 - OR -
third edition, second printing, February 1989 - OR -

 fourth edition, 1st, 2nd, 3rd, or 4th printing, including corrections and changes issued by the AMA prior to May 16, 2000.
fourth edition, 1st, 2nd, 3rd, or 4th printing, including corrections and changes issued by the AMA prior to May 16, 2000.
NOTE: A finding of no impairment is not equivalent to a 0% impairment rating. A doctor can only assign an impairment rating, including a 0% rating, if the doctor performed the examination and testing required by the AMA Guides.
V. DOCTOR’S CERTIFICATION
18.I HEREBY CERTIFY THAT THIS REPORT OF MEDICAL EVALUATION is complete and accurate and complies with the Texas Labor Code and applicable rules. If an impairment rating has been assigned, I certify that I have completed the required training and testing and have a current certification by DWC to assign impairment ratings in the Texas workers' compensation system or have received specific permission by DWC to certify MMI and assign an impairment rating. I understand that making a misrepresentation about a workers’ compensation claim or myself is a crime that can result in fines and/or imprisonment and nullification of this report.
|
Signature of Certifying Doctor: _________________________________________________ |
Date of Certification: __________________ |
|||
|
VI. TREATING DOCTOR’S AGREEMENT OR DISAGREEMENT WITH ANOTHER DOCTOR’S CERTIFICATION |
||||
19. |
Treating Doctor's Name and License Type |
22. |
|
||
|
|
|
|
I AGREE / I DISAGREE with the certifying doctor’s certification of MMI. |
|
20. |
Treating Doctor's License Number and Jurisdiction |
|
23. |
|
|
|
|
|
|
I AGREE / I DISAGREE with the certifying doctor’s finding of no impairment. - OR - |
|
21. |
Treating Doctor’s Phone and Fax Numbers |
|
I AGREE / I DISAGREE with the impairment rating assigned by the certifying doctor. |
||
(Ph) |
(Fax) |
|
|
||
24.I understand that making a misrepresentation about a workers’ compensation claim is a crime that can result in fines and/or imprisonment.
Signature of Treating Doctor: __________________________________________________ |
Date: _____________________________ |
DWC069 Rev. 01/15 |
Page 1 of 3 |
DWC069
Frequently Asked Questions
Report of Medical Evaluation (DWC
INSTRUCTIONS FOR DOCTORS:
Who can file the DWC
Treating Doctor: Doctor chosen by the employee who is primarily responsible for employee's
Doctor Selected by Treating Doctor: Doctor selected by the treating doctor to evaluate permanent impairment and Maximum Medical Improvement (MMI). This doctor acts in the place of the treating doctor. Such a doctor must be selected if the treating doctor is not authorized to certify MMI or assign an impairment rating in those cases in which the employee has permanent impairment. An authorized treating doctor may also choose to select another doctor to perform the evaluation/certification.
Designated Doctor: Doctor selected by the Texas Department of Insurance, Division of Workers’ Compensation (DWC) to resolve a question over MMI or permanent impairment.
Insurance
AUTHORIZATION: In addition to the requirement of acting in an eligible role, 28 Texas Administrative Code §130.1 provides the following requirements:
Employee has permanent impairment: Only a doctor certified by DWC to assign impairment ratings or who receives specific
permission by exception granted by DWC is authorized to certify MMI and to assign an impairment rating.
Employee does not have permanent impairment: A doctor not certified or exempted from certification by DWC is only authorized to determine whether an employee has permanent impairment and, in the event that the employee has no impairment, certify MMI.
INVALID CERTIFICATION: Certification by a doctor who is not authorized is invalid.
Under what circumstances and when am I required to file the DWC
If the employee has reached MMI, you must file the DWC
Where do I file the form?
The DWC
the insurance carrier;
the treating doctor (if a doctor other than the treating doctor files the report);
DWC;
injured employee; and
injured employee’s representative (if any).
The report must be filed by facsimile or electronic transmission unless an exception applies. The specific requirements are shown below. To file this form with DWC, fax to (512)
|
|
Insurance Carrier |
|
Treating Doctor |
|
|
|
DWC |
|
|
|
|
|
|
Designated Doctor |
fax or |
fax or |
||
|
|
|
|
|
Treating Doctor |
|
|
|
fax or |
Doctor Selected by Treating Doctor |
|
fax or |
not provided these numbers; then |
|
Insurance |
|
|
|
by other verifiable means |
Injured Employee
Injured Employee’s Representative
fax or
fax or
Do I have to maintain documentation regarding the examination and report?
The certifying doctor must maintain the original copy of the report and narrative and documentation of the following:
date of the examination;
date any medical records necessary to make the certification of MMI were received, and from whom the medical records were received; and
date, addresses, and means of delivery that required reports were transmitted or mailed by the certifying doctor.
Where can I find more information about the Report of Medical Evaluation?
See 28 TAC §130.1 through §130.4 and §130.6 for the complete requirements regarding the filing of this report, including required documentation. The complete text of these rules is available on the Texas Department of Insurance website at www.tdi.texas.gov/wc/rules/index.html. If you have additional questions, call
DWC069 Rev. 01/15 |
Page 2 of 3 |
DWC069
IMPORTANT INFORMATION FOR INJURED EMPLOYEES:
What if I disagree with the doctor's certification of Maximum Medical Improvement (MMI) and/or permanent impairment rating for my workers' compensation claim?
If this is the first evaluation of your MMI and/or permanent impairment, you or your representative may dispute:
the certification of MMI; and/or
the assigned impairment rating.
To file the dispute, contact your local DWC field office or call
the appointment of a designated doctor (DD), if one has not been appointed; or
a Benefit Review Conference (BRC).
Important Note: Your dispute must be filed within 90 days after the written notice is delivered to you or the certification of MMI and/or the assigned impairment rating may become final.
NOTE: With few exceptions, upon your request, you are entitled to be informed about the information DWC collects about you; receive and review the information (Government Code, §§552.021 and 552.023); and have DWC correct information that is incorrect (Government Code, §559.004).
DWC069 Rev. 01/15 |
Page 3 of 3 |
More PDF Templates
Reseller Permit Texas - Maintaining accurate records of your submitted application will help track your permit status.
Property Tax Exemption for Disabled in Texas - The exemption applies to franchise tax reports due on or after May 1, 1982.
Common mistakes
-
Missing Information: One common mistake is failing to fill out all required fields. Essential details such as the injured employee's name, date of injury, and the certifying doctor's information must be complete. Omitting any of these can delay processing.
-
Incorrect Dates: Providing incorrect dates, particularly for the date of the exam or the date MMI was reached, can lead to complications. Ensure that all dates are accurate and reflect the actual events.
-
Improper Role Selection: Doctors often misidentify their role in the evaluation. It’s crucial to select the correct role, whether it’s treating doctor or designated doctor. Misunderstanding this can invalidate the report.
-
Documentation Issues: Failing to include necessary documentation can be a significant error. This includes not attaching narratives that support the MMI certification or impairment rating. Such omissions can result in disputes or rejections.
Key takeaways
Ensure you have the correct claim numbers before starting the DWC069 form. This includes both the DWC claim number and the carrier claim number.
Gather all general information about the injured employee, including their name, date of injury, and contact information.
Identify your role in the claim clearly. Only authorized doctors can evaluate MMI and file this report.
Document the date of the examination and include relevant diagnosis codes as required.
Determine whether the employee has reached Maximum Medical Improvement (MMI) and provide the date of MMI certification.
If applicable, assess and report any permanent impairment resulting from the compensable injury, including the percentage of impairment.
Complete the doctor’s certification section accurately. Misrepresentation can lead to serious legal consequences.
File the DWC069 form within the required timeframe, specifically within the seventh working day after the examination or receipt of necessary medical records.
Maintain all relevant documentation related to the examination and report for your records.
Steps to Using Texas Dwc069
Completing the Texas DWC069 form is a critical step in the workers' compensation process. This form must be filled out accurately to ensure that the injured employee receives the appropriate medical evaluation and benefits. Here are the steps to fill out the form correctly.
- Begin with the General Information. Fill in the Workers’ Compensation Insurance Carrier, Employer’s Name, and Employer’s Address.
- Provide the Injured Employee's Name, Date of Injury, and Social Security Number.
- Enter the Employee's Phone Number and Address.
- Complete the Certifying Doctor's Name, License Type, License Number, and Jurisdiction.
- Include the Certifying Doctor’s Phone and Fax Numbers, along with their Address.
- Move to the Doctor’s Role section. Indicate the role you are serving in the claim by selecting one of the provided options.
- In the Medical Status Information section, enter the Date of Exam and Diagnosis Codes.
- Indicate whether the employee has reached Clinical or Statutory MMI. Provide the date and attach any necessary documentation.
- If applicable, complete the Permanent Impairment section. State whether the employee has permanent impairment and provide the percentage if applicable.
- In the Doctor’s Certification section, certify that the report is complete and accurate. Sign and date the form.
- If there is a Treating Doctor, fill out their information and indicate whether they agree or disagree with the certifying doctor’s findings.
- Finally, ensure all required documentation is attached and that the form is filed with the necessary parties.