Blank Texas 3599 PDF Template
Form Example
Texas Department of Aging |
Community Living Assistance and Support Services (CLASS) |
|
and Disability Services |
|
|
|
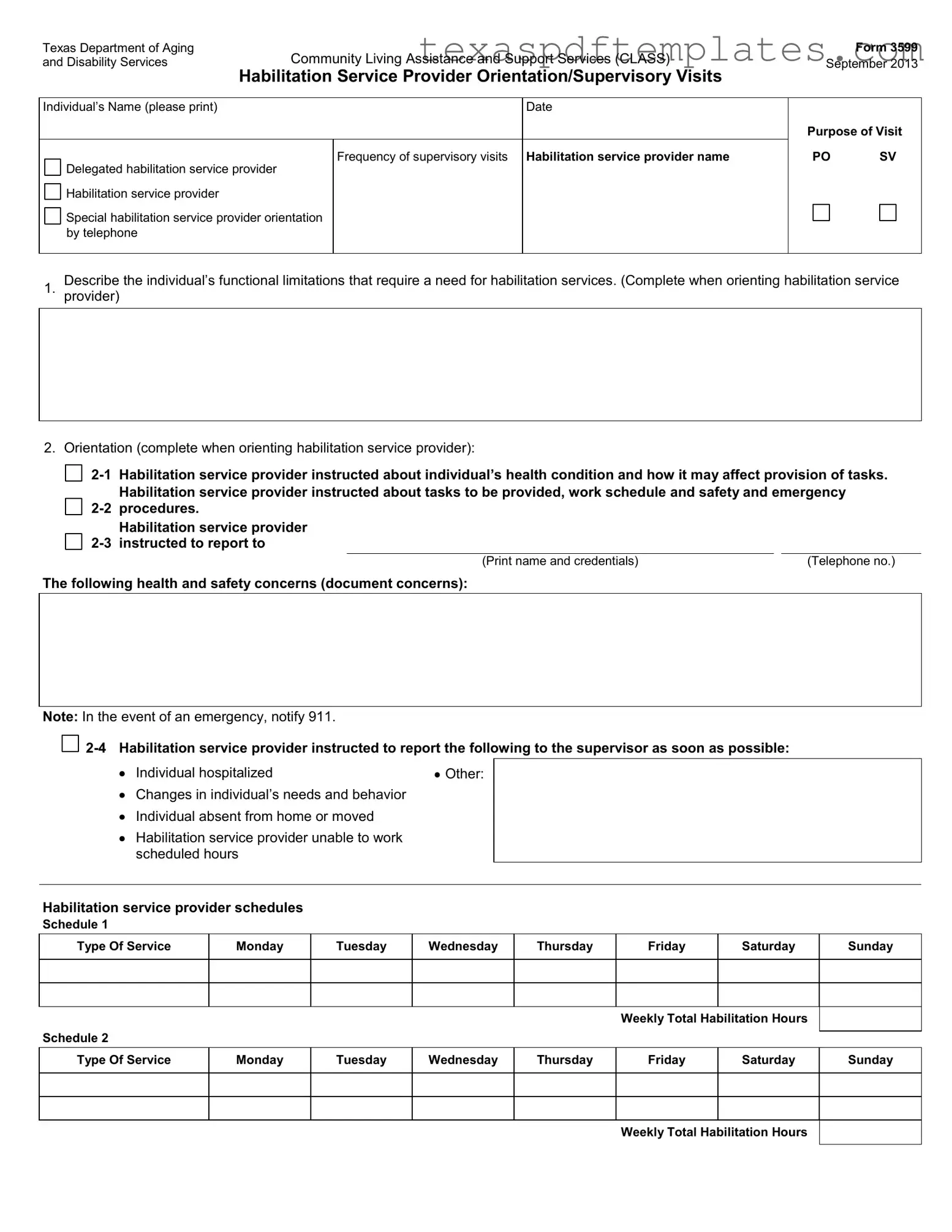
Habilitation Service Provider Orientation/Supervisory Visits |
|
|
|
|
Individual’s Name (please print) |
Date |
|
|
|
|
|
Frequency of supervisory visits Habilitation service provider name |
|
Delegated habilitation service provider |
|
|
Habilitation service provider |
|
|
Special habilitation service provider orientation by telephone
Form 3599
September 2013
Purpose of Visit
PO SV
Describe the individual’s functional limitations that require a need for habilitation services. (Complete when orienting habilitation service
1. provider)
2. Orientation (complete when orienting habilitation service provider):
Habilitation service provider instructed about individual’s health condition and how it may affect provision of tasks. |
||||
|
Habilitation service provider instructed about tasks to be provided, work schedule and safety and emergency |
|||
procedures. |
|
|
||
|
Habilitation service provider |
|
|
|
instructed to report to |
|
|
||
|
|
|
|
|
|
|
(Print name and credentials) |
|
(Telephone no.) |
The following health and safety concerns (document concerns):
Note: In the event of an emergency, notify 911.


Individual hospitalized |
Other: |
 Changes in individual’s needs and behavior
Changes in individual’s needs and behavior
 Individual absent from home or moved
Individual absent from home or moved
 Habilitation service provider unable to work scheduled hours
Habilitation service provider unable to work scheduled hours
Habilitation service provider schedules
Schedule 1
Type Of Service |
Monday |
Tuesday |
Wednesday |
Thursday |
Friday |
Saturday |
Sunday |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Weekly Total Habilitation Hours
Schedule 2
Type Of Service
Monday
Tuesday
Wednesday
Thursday
Friday
Saturday
Sunday
Weekly Total Habilitation Hours
Form 3599
Page 2 /
Individual’s Name (please print)
3.A. Tasks/Plan of Care: Indicate tasks to be performed (complete on every visit). During supervisory visit, ask individual or LAR what tasks are provided by the service provider. Observe or ask about performance: S = Satisfactory U = Unsatisfactory
Hygiene..............
Toileting.............
Dressing.............
Shopping ...........
Meal Preparation
Freq. Perform.
Feeding ..........................
Exercise .........................
Transfer/Ambulation......
Cleaning .........................
Community Assistance
Freq. Perform.
Medically Related Tasks......
Freq. Perform.
3.B. Is the habilitation service provider competent to provide habilitation tasks? |
Yes |
|
|
3.C. Is the habilitation service provider competent to provide delegated habilitation tasks? |
Yes |
|
3.D. Is the habilitation service provider competent to provide medically related tasks? |
Yes |
Complete the following for Supervisory Visits (N/A for habilitation service provider orientation only).
4. |
Is the individual satisfied with the services provided by the habilitation service provider? |
Yes |
|
||
5. |
Is the habilitation service provider following the schedule? |
Yes |
6.A. |
Describe service delivery problems. |
|
No
No
No
No No
N/A
N/A
N/A
6.B. Describe habilitation service provider training needs.
6.C. Describe corrective actions taken.
7. Does the individual continue to need services? ...........................................................................................................
8. Additional Comments:
Yes
No
Signature – Individual/LAR |
|
Date |
|
|
|
Signature – Habilitation Service Provider |
|
Date |
|
|
|
Signature – Supervisor |
|
Date |
More PDF Templates
Register Car in Texas - All applications should be forwarded to the Texas Department of Transportation in Austin.
How to Know If I Have Medicaid - Birth dates, social security numbers, and contact information will be requested on the form.
How to Get a Drivers License in Texas at 16 - The form also requires adult supervision, which helps in reinforcing safe driving habits.
Common mistakes
-
Failing to provide the individual's name clearly. This can lead to confusion about who the form is for.
-
Not including the date of the visit. Without a date, tracking the service history becomes difficult.
-
Leaving the frequency of supervisory visits section blank. This information is crucial for scheduling and accountability.
-
Inaccurately describing the individual’s functional limitations. This can affect the services provided and their effectiveness.
-
Neglecting to document health and safety concerns. This oversight can jeopardize the individual's well-being.
-
Not specifying the tasks to be performed during each visit. Clear task descriptions ensure proper care and accountability.
-
Failing to assess the competence of the habilitation service provider. This evaluation is essential for quality service delivery.
-
Omitting the signature of the individual or their legally authorized representative (LAR). Signatures validate the document and its contents.
-
Ignoring the additional comments section. This area can provide valuable insights or clarifications about the service.
Key takeaways
- Form Purpose: The Texas 3599 form is used for documenting supervisory visits and orientations for habilitation service providers.
- Individual Identification: Always print the individual's name clearly at the top of the form.
- Frequency of Visits: Specify how often supervisory visits will occur to ensure consistent support.
- Functional Limitations: Clearly describe the individual's functional limitations that necessitate habilitation services.
- Health and Safety Instructions: Provide detailed instructions regarding the individual’s health conditions and any relevant safety procedures.
- Emergency Protocol: In case of emergencies, it is crucial to notify 911 immediately.
- Task Performance Evaluation: Document whether tasks performed by the habilitation service provider are satisfactory or unsatisfactory during each visit.
- Competency Assessment: Confirm the habilitation service provider's competency in providing required tasks, including medically related tasks.
- Service Satisfaction: Assess the individual's satisfaction with the services provided by the habilitation service provider.
- Corrective Actions: Note any service delivery problems and outline corrective actions taken to address them.
Steps to Using Texas 3599
Completing the Texas 3599 form is an important step in documenting the habilitation services provided to individuals. This form captures essential information about the individual's needs, the services rendered, and the provider's performance. Follow these steps to ensure accurate completion of the form.
- Print the individual’s name at the top of the form.
- Fill in the date of the supervisory visit.
- Indicate the frequency of supervisory visits in the designated space.
- Write the name of the habilitation service provider and the delegated habilitation service provider.
- Document the health and safety concerns that need to be reported during the visit.
- Complete the tasks/plan of care section by indicating the tasks to be performed and their frequency.
- Assess the competency of the habilitation service provider for habilitation tasks, delegated tasks, and medically related tasks. Mark "Yes" or "No" as appropriate.
- Record the individual's satisfaction with the services provided and whether the provider is following the schedule.
- Describe any service delivery problems and the training needs of the habilitation service provider.
- Document any corrective actions that have been taken.
- Indicate if the individual continues to need services by marking "Yes" or "No."
- Add any additional comments that may be relevant.
- Sign and date the form at the bottom by the individual or their legally authorized representative, the habilitation service provider, and the supervisor.
After completing the form, ensure that all sections are filled out clearly and accurately. This documentation is vital for maintaining high-quality care and meeting regulatory requirements.