Blank Texas 1560 PDF Template
Form Example
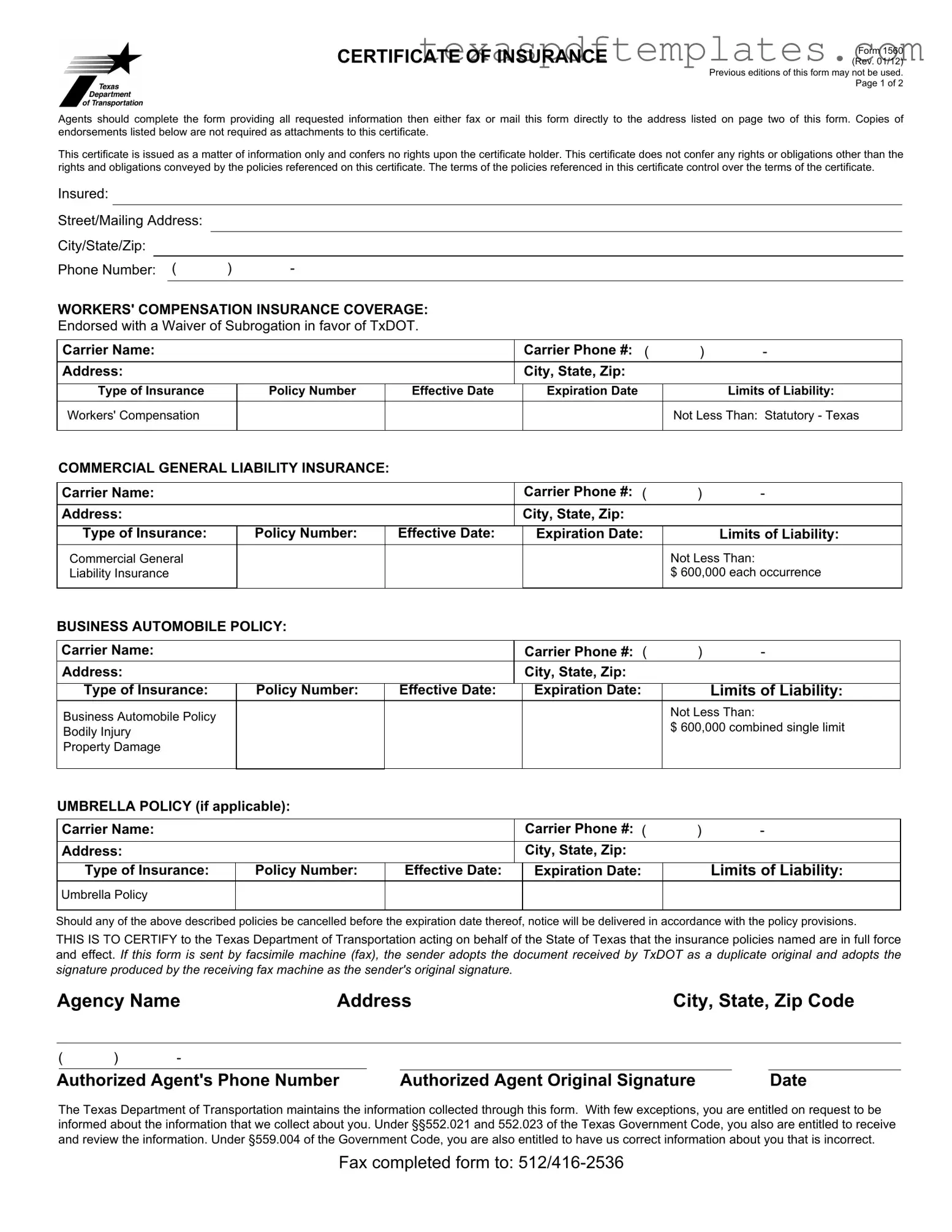
CERTIFICATE OF INSURANCE
Form 1560 (Rev. 01/12)
Previous editions of this form may not be used. Page 1 of 2
Agents should complete the form providing all requested information then either fax or mail this form directly to the address listed on page two of this form. Copies of endorsements listed below are not required as attachments to this certificate.
This certificate is issued as a matter of information only and confers no rights upon the certificate holder. This certificate does not confer any rights or obligations other than the rights and obligations conveyed by the policies referenced on this certificate. The terms of the policies referenced in this certificate control over the terms of the certificate.
Insured:
Street/Mailing Address:
City/State/Zip:
Phone Number: ( |
) |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
WORKERS' COMPENSATION INSURANCE COVERAGE: |
|
|
|
|
||||||
Endorsed with a Waiver of Subrogation in favor of TxDOT. |
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
Carrier Name: |
|
|
|
|
|
Carrier Phone #: ( |
) |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
City, State, Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Type of Insurance |
|
Policy Number |
|
Effective Date |
Expiration Date |
|
Limits of Liability: |
|||
|
|
|
|
|
|
|
|
|
||
Workers' Compensation |
|
|
|
|
|
|
Not Less Than: Statutory - Texas |
|||
|
|
|
|
|
|
|
|
|
||
COMMERCIAL GENERAL LIABILITY INSURANCE: |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
Carrier Name: |
|
|
|
|
|
Carrier Phone #: ( |
) |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
City, State, Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Type of Insurance: |
|
Policy Number: |
|
Effective Date: |
Expiration Date: |
|
Limits of Liability: |
|||
|
|
|
|
|
|
|
|
|
||
Commercial General |
|
|
|
|
|
|
Not Less Than: |
|||
Liability Insurance |
|
|
|
|
|
|
$ 600,000 each occurrence |
|||
|
|
|
|
|
|
|
|
|
||
BUSINESS AUTOMOBILE POLICY: |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
Carrier Name: |
|
|
|
|
|
Carrier Phone #: ( |
) |
- |
|
|
Address: |
|
|
|
|
|
City, State, Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Type of Insurance: |
|
Policy Number: |
|
Effective Date: |
Expiration Date: |
|
Limits of Liability: |
|
||
Business Automobile Policy |
|
|
|
|
|
|
Not Less Than: |
|
||
|
|
|
|
|
|
$ 600,000 combined single limit |
|
|||
Bodily Injury |
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
||
Property Damage |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
UMBRELLA POLICY (if applicable): |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
Carrier Name: |
|
|
|
|
|
Carrier Phone #: ( |
) |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
City, State, Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Type of Insurance: |
|
Policy Number: |
|
Effective Date: |
Expiration Date: |
|
Limits of Liability: |
|
||
|
|
|
|
|
|
|
|
|
|
|
Umbrella Policy |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Should any of the above described policies be cancelled before the expiration date thereof, notice will be delivered in accordance with the policy provisions.
THIS IS TO CERTIFY to the Texas Department of Transportation acting on behalf of the State of Texas that the insurance policies named are in full force and effect. If this form is sent by facsimile machine (fax), the sender adopts the document received by TxDOT as a duplicate original and adopts the signature produced by the receiving fax machine as the sender's original signature.
Agency Name |
Address |
City, State, Zip Code |
|||||
|
|
|
|
|
|
|
|
( |
) |
- |
|
|
|
|
|
|
|
|
|
||||
Authorized Agent's Phone Number |
Authorized Agent Original Signature |
|
Date |
||||
The Texas Department of Transportation maintains the information collected through this form. With few exceptions, you are entitled on request to be informed about the information that we collect about you. Under §§552.021 and 552.023 of the Texas Government Code, you also are entitled to receive and review the information. Under §559.004 of the Government Code, you are also entitled to have us correct information about you that is incorrect.
Fax completed form to:

Form 1560 (Rev. 01/12) Page 2 of 2
NOTES TO AGENTS:
Agents must provide all requested information then either fax or mail this form directly to the address listed below.
To avoid work suspension, an updated insurance form must reach the address listed below one business day prior to the expiration date. Insurance must be in force in order to perform any work.
Binder numbers are not acceptable for policy numbers.
The certificate of insurance, once on file with the department, is adequate for subsequent department contracts provided adequate coverage is still in effect. Do not refer to specific projects/contracts on this form.
List the contractor's legal company name, including the DBA (doing business as) name as the insured. If a staff leasing service is providing insurance to the contractor/client company, list the staff leasing service as the insured and show the contractor/client company in parenthesis.
The TxDOT certificate of insurance form is the only acceptable proof of insurance for department contracts.
List the contractor's legal company name, including the DBA (doing business as) name as the insured or list both the contractor and staff leasing service as insured when a staff leasing service is providing insurance.
This form may be reproduced.
DO NOT COMPLETE THIS FORM UNLESS THE WORKERS' COMPENSATION POLICY IS ENDORSED WITH A WAIVER OF SUBROGATION IN FAVOR OF TXDOT.
The SIGNATURE of the agent is required.
CERTIFICATE OF INSURANCE REQUIREMENTS:
WORKERS' COMPENSATION INSURANCE:
The contractor is required to have Workers' Compensation Insurance if the contractor has any employees including relatives.
The word STATUTORY, under limits of liability, means that the insurer would pay benefits allowed under the Texas Workers' Compensation Law.
GROUP HEALTH or ACCIDENT INSURANCE is not an acceptable substitute for Workers' Compensation.
COMMERCIAL GENERAL LIABILITY INSURANCE:
MANUFACTURERS' or CONTRACTOR LIABILITY INSURANCE is not an acceptable substitute for Comprehensive General Liability Insurance or Commercial General Liability Insurance.
BUSINESS AUTOMOBILE POLICY:
If coverages are specified separately, they must be at least these amounts:
Bodily Injury |
$500,000 each occurrence |
|
$100,000 each occurrence |
Property Damage |
$100,000 for aggregate |
PRIVATE AUTOMOBILE LIABILITY INSURANCE is not an acceptable substitute for a Business Automobile Policy.
MAIL ALL CERTIFICATES TO:
Texas Department of Transportation
CST Contract Processing Unit (RA/200 1st Fl.) 125 E. 11th Street
Austin, TX
More PDF Templates
How to Get a Birth Certificate in Texas Without Id - A new birth certificate can be filed for corrections to a child's name or sex.
Texas Workforce Commission Quarterly Report Forms Pdf - Employers need to report the amounts as originally stated and the correct amounts.
Common mistakes
-
Incomplete Information: Failing to fill in all required fields can delay processing. Ensure every section, including the insured's name, address, and contact information, is complete.
-
Incorrect Policy Numbers: Entering binder numbers instead of actual policy numbers is a common mistake. Only valid policy numbers should be listed to avoid rejection.
-
Missing Waiver of Subrogation: Not endorsing the Workers' Compensation policy with a waiver of subrogation in favor of TxDOT can lead to issues. This endorsement is mandatory.
-
Using Outdated Forms: Submitting previous editions of the form is unacceptable. Always use the most current version, as specified in the instructions.
-
Inaccurate Limits of Liability: Providing lower limits than those required can result in non-compliance. Ensure that limits meet or exceed the minimum specified amounts.
-
Improper Signature: The agent's original signature is necessary. Digital signatures or stamps may not suffice, leading to potential delays.
-
Neglecting to Update Before Expiration: Failing to submit an updated form at least one business day before the expiration date can cause work suspension. Timely submission is crucial.
Key takeaways
Here are key takeaways for using the Texas 1560 form:
- Complete All Sections: Ensure that every requested field is filled out accurately. Missing information can lead to delays.
- Submit Correctly: After completing the form, either fax or mail it directly to the specified address. Do not send it to any other location.
- Understand the Coverage: The form certifies that the insurance policies are active. However, it does not confer any additional rights beyond what is stated in the policies.
- Use the Right Limits: Minimum required limits are pre-printed. If your policy offers higher limits, enter those and cross out the minimums.
- Timely Updates: Submit an updated form at least one business day before your current insurance expires to avoid work interruptions.
- Follow Signature Requirements: The authorized agent must sign the form. If faxed, the faxed signature is considered an original.
Steps to Using Texas 1560
After gathering all necessary information, proceed to fill out the Texas 1560 form. Ensure that all details are accurate and complete before submitting the form to the Texas Department of Transportation.
- Identify the Insured: Enter the legal name of the contractor or company as the insured. If applicable, include the "doing business as" (DBA) name.
- Provide Address: Fill in the street or mailing address, city, state, and zip code of the insured.
- Enter Phone Number: Include the phone number of the insured in the specified format.
- Workers' Compensation Insurance: Provide the carrier name, phone number, and address. Fill in the type of insurance, policy number, effective date, expiration date, and limits of liability (not less than statutory - Texas).
- Commercial General Liability Insurance: Repeat the process for this section, entering the carrier name, phone number, address, type of insurance, policy number, effective date, expiration date, and limits of liability (not less than $600,000 each occurrence).
- Business Automobile Policy: Enter the carrier name, phone number, address, type of insurance, policy number, effective date, expiration date, and limits of liability (not less than $600,000 combined single limit).
- Umbrella Policy (if applicable): If an umbrella policy exists, provide the carrier name, phone number, address, type of insurance, policy number, effective date, expiration date, and limits of liability.
- Certification: Confirm that the insurance policies named are in full force and effect. Ensure the agent's name, address, phone number, and original signature are included.
- Date: Finally, include the date of completion.
Once completed, either fax or mail the form to the Texas Department of Transportation at the address specified on the form. Ensure that the submission is made timely to avoid any disruptions in work.